From cows to coronavirus and the museum's collection.
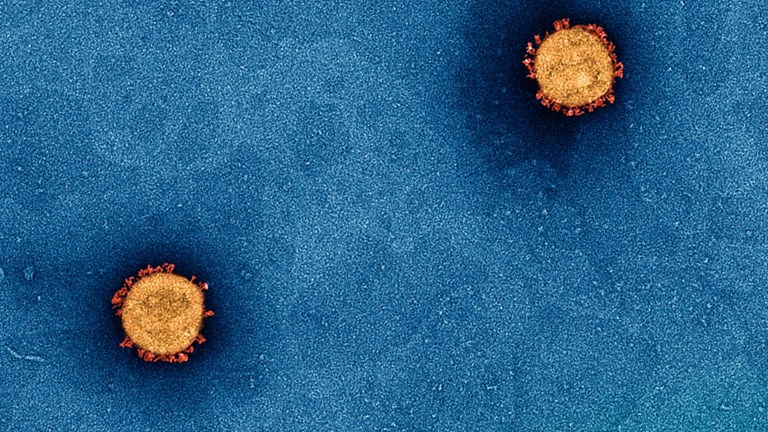
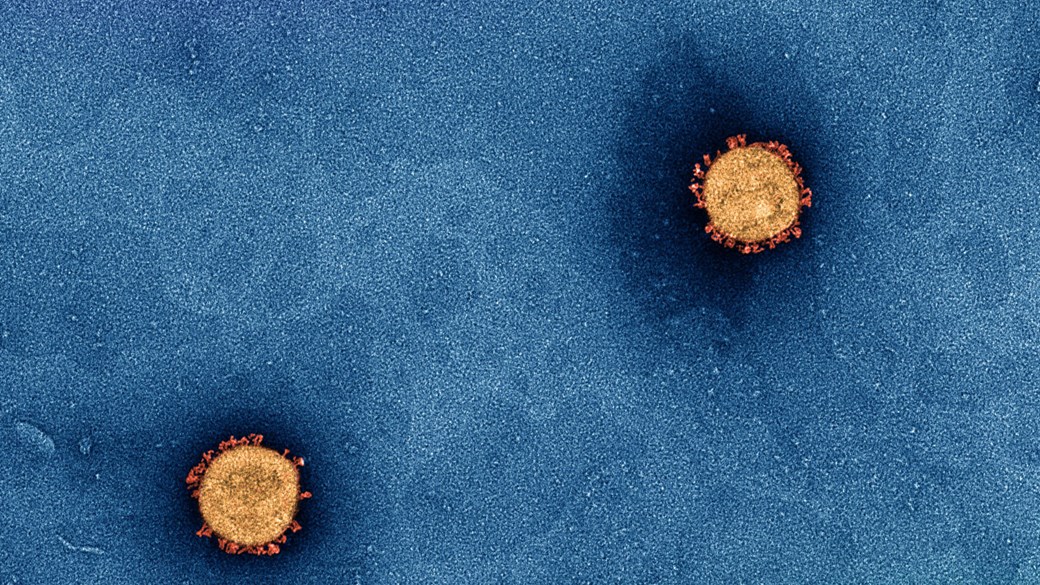
Banner image: Copyright Doherty Institute for Infection and Immunity 2020 Photographer: Dr Jason Roberts; Electron Microscopist: Dr Andrew Leis
Please note: this article features graphic images of people suffering from smallpox and measles.
Museums are used to collecting the artefacts of major world events but actively participating in them is not so common.
In 2021, the Melbourne Museum did just that—becoming a vaccination hub in response to the COVID-19 pandemic.
This is the same building that houses extensive collections of medical breakthroughs, including vaccines developed over the last 100 years.
So, how has that history of vaccine development for previous pandemics shaped our response to this one?
And what will these new collections teach societies of the future?
A world without vaccines would be very different to the one we have today—and more dangerous.
Vaccines are ‘our single most important medical intervention that has saved more lives than anything else,’ says Professor Marc Pellegrini, joint division head of infectious disease and immune defence at WEHI.
In a nutshell, vaccines educate your immune system by stimulating an immune response without giving you the full disease.
This allows your immune system to recognise, and fight against, the real invader if you are ever exposed to it.
It is easy to take for granted just how vital these medical marvels have been for humankind in reducing child mortality and improving our quality and longevity of life.
When we really need vaccines, but don’t have them, we are incredibly vulnerable—a situation acutely felt with the outbreak of COVID-19.
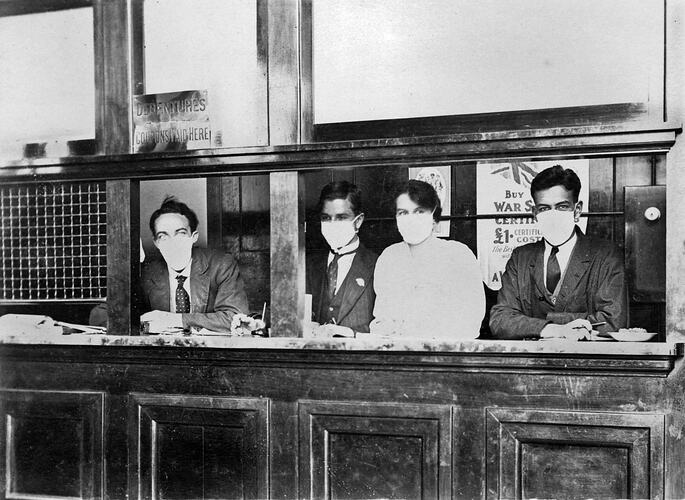
With no other option, those early days of the pandemic necessitated a return to masks and physical distancing to reduce disease transmission.
It was a similar story 100 years ago during the 1918 influenza pandemic, commonly (but unfairly) referred to as the Spanish flu.
MM 135982 –
Bank Tellers Wearing Face Masks, Victoria, 1919
The major difference, though, is that scientists today know what they are fighting against.
Part of the vaccine history collection at Museums Victoria. Photo: Photographer: Michelle McFarlane/Museums Victoria
Influenza
When the influenza pandemic first emerged at the end of World War I in 1918, no one understood what caused it.
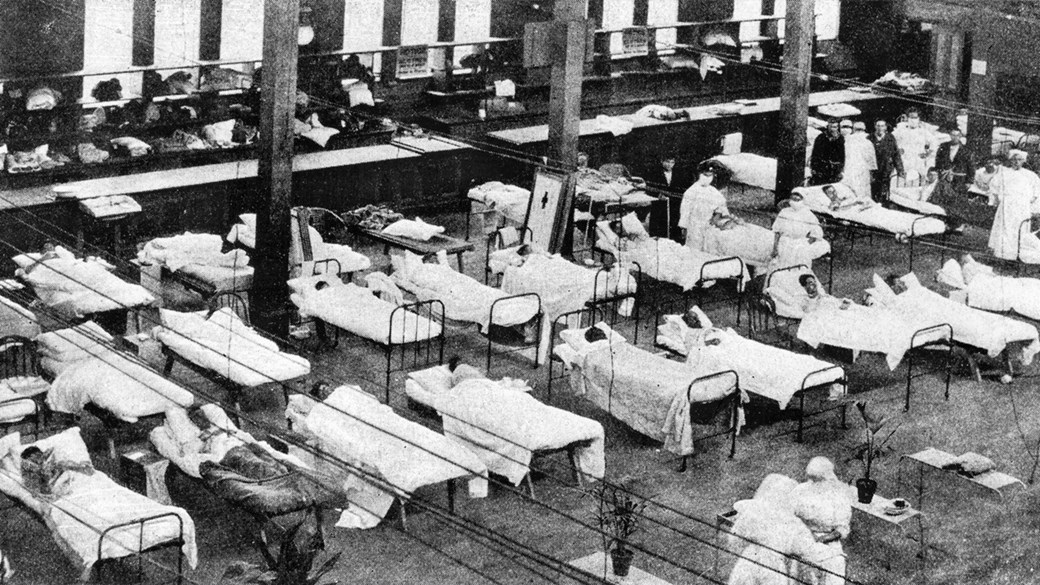
‘Cinemas, schools, racecourses and even state borders were closed in an unsuccessful attempt to halt the spread,’ says Dr Johanna Simkin, senior curator of human biology and medicine at Museums Victoria.
‘Hospitals were overwhelmed, and Melbourne’s Royal Exhibition Building was turned into a temporary hospital.’
A vaccine was quickly developed, but scientists at this time didn’t know that influenza was caused by a virus.
The vaccine was instead made to target bacterial infections and did not address the virus.
It was not until 1933 that scientists first identified the flu virus in an H1N1-type strain.
H1N1 viruses have been behind everything from worldwide pandemics (including in 1918, 1977 and 2009) to seasonal flu.
‘The flu is one of those that is able to mutate quite easily,’ says Dr Simkin.
Dr Johanna Simkin manages Museum Victoria's health and medicine collection.
Scientists constantly monitor outbreaks at worldwide surveillance centres and alter vaccines accordingly: ‘That's why we all need to get our vaccines every year.’
And, as we will later learn, mutation of a pathogen can work both for and against us.
While it is impossible to know exactly how many died in the 1918-19 pandemic, estimates vary between about one and five per cent of the world’s population of 1.8 billion people.
If the same thing were to happen today, that would equate to nearly 400 million deaths—the combined populations of France and the USA.
So, it is a good thing we have become a lot better at making flu vaccines.
But that’s not to say all vaccines before the 1918 flu were impotent; the first vaccine ever created was so successful that we no longer have to worry about that disease at all.
Hospital beds line the Exhibition Building's great hall during the influenza pandemic in 1919. Photo: Museum Victoria
Small Pox
COVID-19 nearly brought the world to a standstill and has dominated daily aspects of our lives.
But as horrible as this disease is, smallpox was another matter entirely.
A girl with smallpox in 1890.
Once the ‘scourge of the human species’, the earliest physical evidence for smallpox is found in scars of mummified Egyptian pharaohs 3,000 years ago but it is believed to be much more ancient.
Patients would come down with a fever, flu-like symptoms and a distinctive skin rash that progressed to fluid-filled blisters.
It killed nearly a third of everyone it infected, and left survivors badly scarred.
Messengers from First Peoples clans travelled to warn their neighbours of the disease but, in doing so, unknowingly spread smallpox themselves.
It devastated entire communities, particularly along river systems.
Elderly people told European observers the death toll was so high in some cases that their dead could not be buried.
The first real attempt to fight against smallpox came in the form of variolation—the precursor to vaccination.
It involved exposing someone to the puss of a smallpox wound, hopefully giving them a mild case of the disease.
After they recovered, most would have long-lasting immunity but the variolation process carried its own risks.
So, when an English doctor named Edward Jenner discovered a more effective, and safer way, people really took notice.
‘Like all good scientific discoveries, it came about by accident,’ says Dr Simkin.
Jenner observed that milkmaids who had been infected with cowpox appeared immune to smallpox.
He tested this theory in 1796 by inoculating an eight-year-old farm hand, James Phipps, with cowpox before exposing him to smallpox.
Fortunately for James, and the rest of us, it worked.
Jenner named the treatment vaccination (from vacca, Latin for cow) and in 1801 wrote: ‘The annihilation of the smallpox, the most dreadful scourge of the human species, must be the final result of this practice’.
And Jenner was right in his prediction but it took 179 years and a concerted effort to get there.
His vaccine quickly spread around the world, replacing variolation as the preferred method of combatting smallpox.
Dr Jenner performing his first vaccination on James Phipps on 14 May, 1796, as painted by Ernest Board. Source: Wellcome Collection
‘That vaccine was incredibly brilliant,’ says Professor Pellegrini.
Keep in mind, this was more than 60 years before scientists established that disease was caused by microbes invading the body (germ theory).
Jenner himself had no idea of the minute scale on which his invention worked.
Scaling the invisible. Animator: Len Doublet, Museums Victoria.
Victoria introduced a Compulsory Vaccination Act in 1854, which largely mitigated the threat and prevented major outbreaks.
The country’s last confirmed case of smallpox was during World War I, but Australians continued to be vaccinated for decades thereafter—many people alive today still carry the tell-tale scar from their immunisation.
‘It’s really important to keep up vaccination levels until you're sure that the disease does not exist anymore,’ says Dr Simkin.
‘There’s a reason that we still have vaccine regimens for all kids and adults.’
The disease remained a serious problem for many nations throughout much of the 1900s but in May 1980, the World Health Organisation announced the death of smallpox to the world.
Smallpox is so far the only human disease we have managed to conquer and this was only possible through vaccination.
We are close to eradicating other diseases, but as Professor Pellegrini says: ‘We've been saying we’re close to [eliminating polio] for the last 20 years.
‘To actually eliminate a virus requires virtually 100 per cent immunisation.’
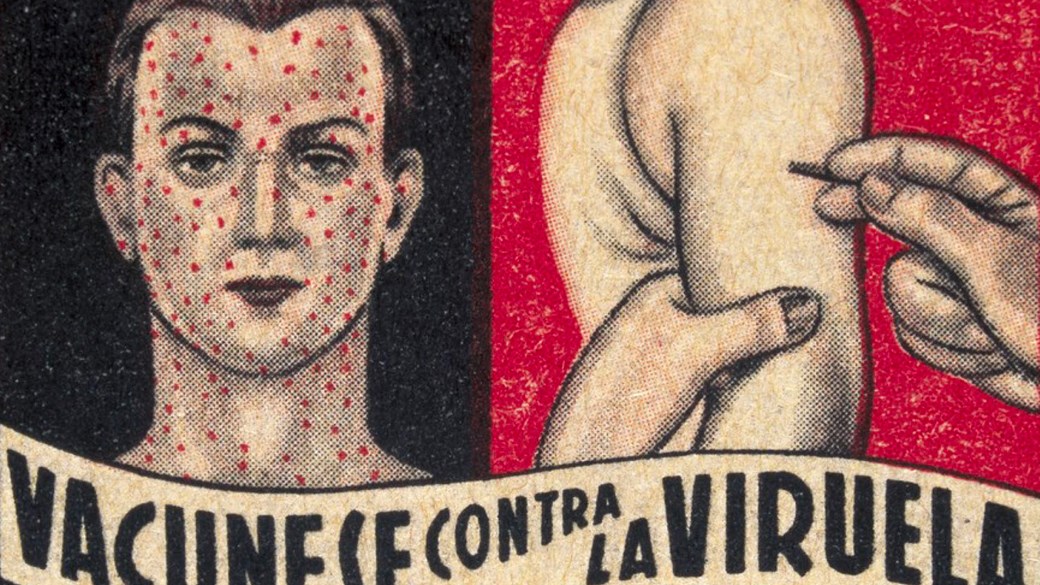
This Spanish advertisement from the 1940s reads 'get vaccinated against smallpox'. Source: Wellcome collection
Polio
Like smallpox, there are few people alive in the developed world today who truly know the horrors of polio, again, thanks to vaccination.
Polio, or poliomyelitis, is highly infectious and predominantly affects children under the age of five.
Most people infected show no symptoms but in one in every 200 cases the virus attacks the nervous system, causing permanent paralysis.
Up to one in ten of those paralysed die because their breathing muscles have stopped responding.
An iron lung surrounded the patient’s body, except for their head, creating a vacuum that pumped air in and out of their lungs. A mirror mounted above the head allowed patients to see their surroundings.
The saviour of many polio patients came in the shape of a coffin-like machine, known as an iron lung.
Many people who survived polio required the use of an iron lung for the rest of their lives.
There was a time when thousands of them filled hospitals across the world but, fortunately, the most likely place you’ll find an iron lung now is in a museum.
One of the biggest issues with the development of vaccines for any disease, explains Dr Simkin, is funding.
‘Even back then—can you get media coverage to get people interested enough to give researchers the money, so they can actually do the research?
‘If a rich population is being particularly affected by something, generally that rich population puts money into developing a cure.’
In the case of polio, that population was the United States of America and among those diagnosed was a president.
Roosevelt was rarely seen in his wheelchair, but he publicly championed the cause of polio patients.
Franklin D Roosevelt was paralysed below the waist at age 39 and it was his advocacy and fundraising efforts that led to the development of two vaccines.
Some children with polio suffered muscle paralysis. Crutches and braces took on the work of paralysed muscles to keep legs straight. Photo: Winton Irving/Copyright Northcott Disability Services
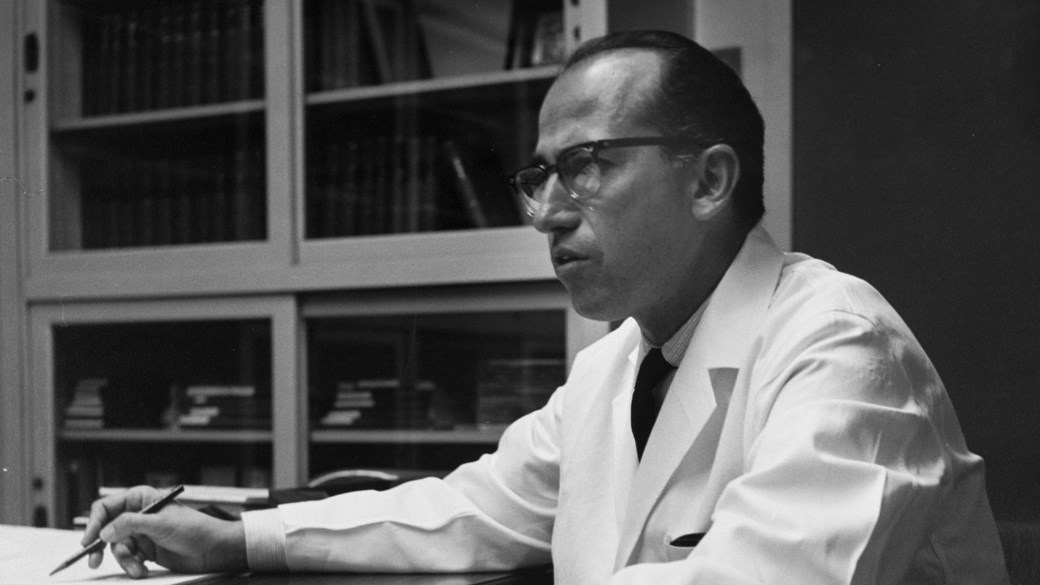
American virologist Dr Jonas Salk was the first to develop a safe and effective vaccine against polio, using an inactivated virus—a technique he learned from researching the flu virus.
At the time, the most prominent view was that only a live virus could stimulate the immune system to recognise and fight polio.
But Salk didn’t want to risk infecting the patient and took the unusual step killing the virus in a formaldehyde solution.
He announced his vaccine was ready for trials in 1953 but it took two years before it was finally approved for use.
Before the vaccine’s release in the US, there was an average of 45,000 cases every year but by 1962 there were just 910—Salk was hailed as a hero.
It reduced the number of cases 20-fold in the space of 12 months.
But Salk’s vaccine had its limitations.
Jonas Salk Photo: Theodore Hall Collection/San Diego Air and Space Museum Archive
In Australia herd immunity was not reached quickly enough and by 1961 there was another outbreak.
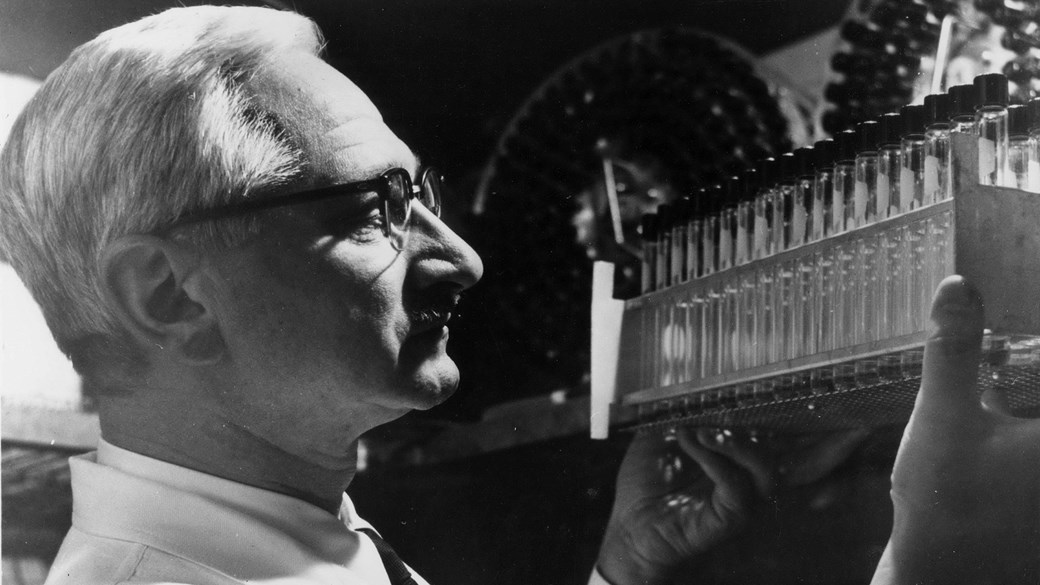
A rival of Salk’s, Dr Albert Sabin, developed his own attenuated live virus vaccine that could be administered orally, provided longer-lasting immunity, and was much cheaper to manufacture.
It took over as the preferred vaccine in global eradication efforts and is responsible for much of polio’s decline.
Australia hasn’t had a case since 1979, while the USA has been polio-free since 1994.
Albert Sabin. Source: Courtesy Hauck Center for the Albert B. Sabin Archives, Henry R. Winkler Center for the History of the Health Professions, University of Cincinnati Libraries
However, in extremely rare cases (one in 2.7 million doses) the live virus in Sabin’s vaccine can mutate and cause a case of a paralytic polio.
It is for this reason that the World Health Organisation has recommended a return to using the killed virus vaccine.
According to the World Health Organisation: ‘Failure to eradicate polio from these last remaining strongholds could result in as many as 200,000 new cases every year, within 10 years, all over the world.’
And we have reason to be concerned about that possibility because when vaccination rates drop, some diseases come back with a vengeance.
Whooping Cough
Pertussis (or whooping cough) is wildly infectious, debilitating, and difficult to treat but, importantly, preventable.
An effective vaccine was first produced the 1940s and has been steadily improved since—it is now found in a combined vaccine with diphtheria and tetanus.
Unfortunately, the whooping cough vaccine has also been the target of the anti-vaccine movement which has caused the disease’s resurgence in several countries.
Pertussis seemed well under control up until the 1970s, when a misleading reportlinked the vaccine to neurological damage in children—a condition later proven not to be related to vaccines butinfantile epilepsy.
The United Kingdom, Sweden and Japan subsequently decreased their vaccination programs and all experienced whooping cough epidemics.
Australia’s vaccination rates followed suit, not because of a change in government policy but, because of misinformation.
It was enough to give whooping cough a foothold and now it is one of the leading causes of vaccine-preventable deaths around the world.
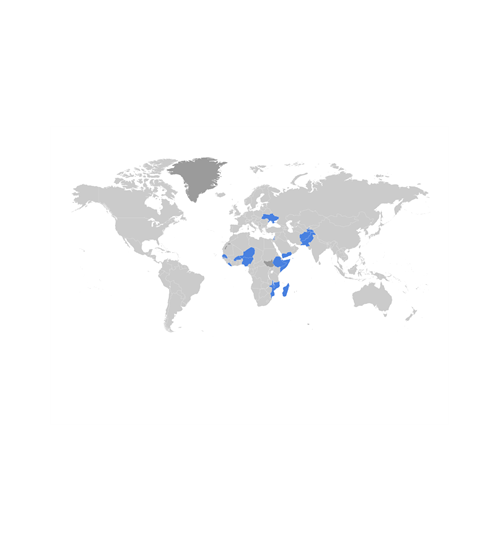
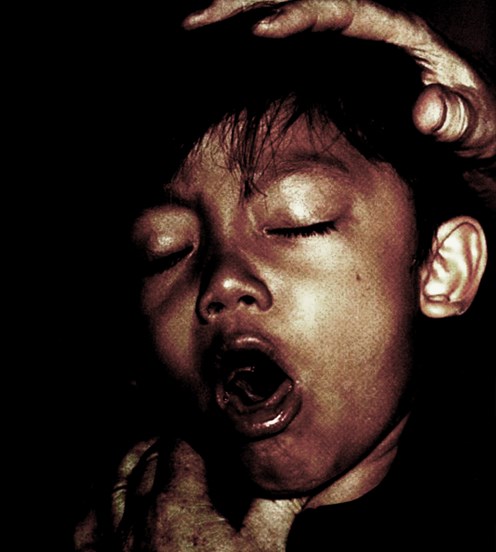
A young boy is presented to a clinic suffering from what was diagnosed as pertussis. Source: Centers for Disease Control/Public Health Image Library
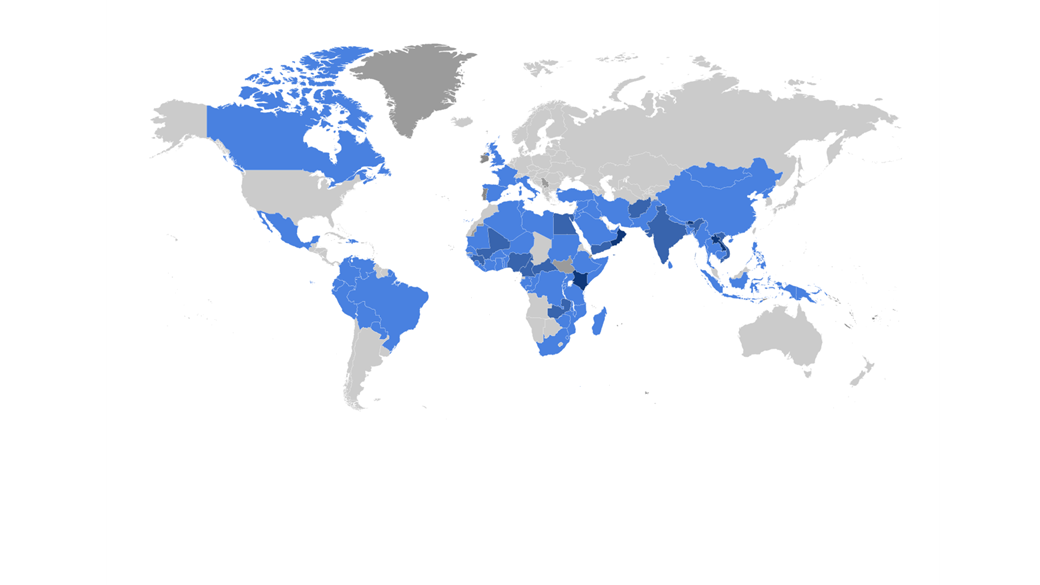
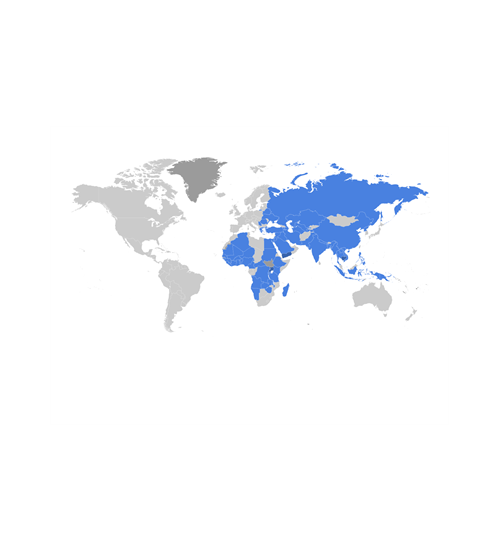
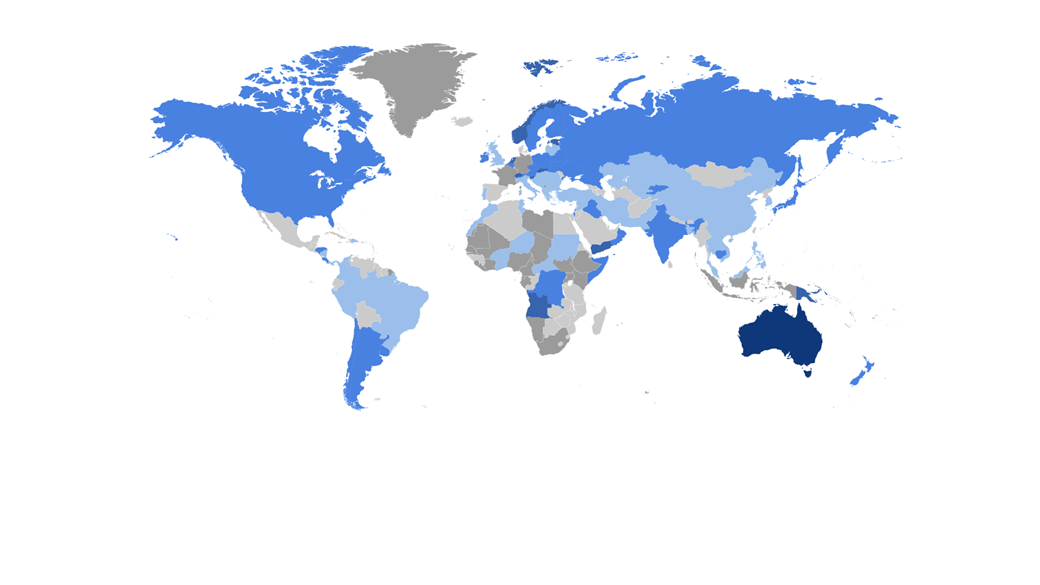
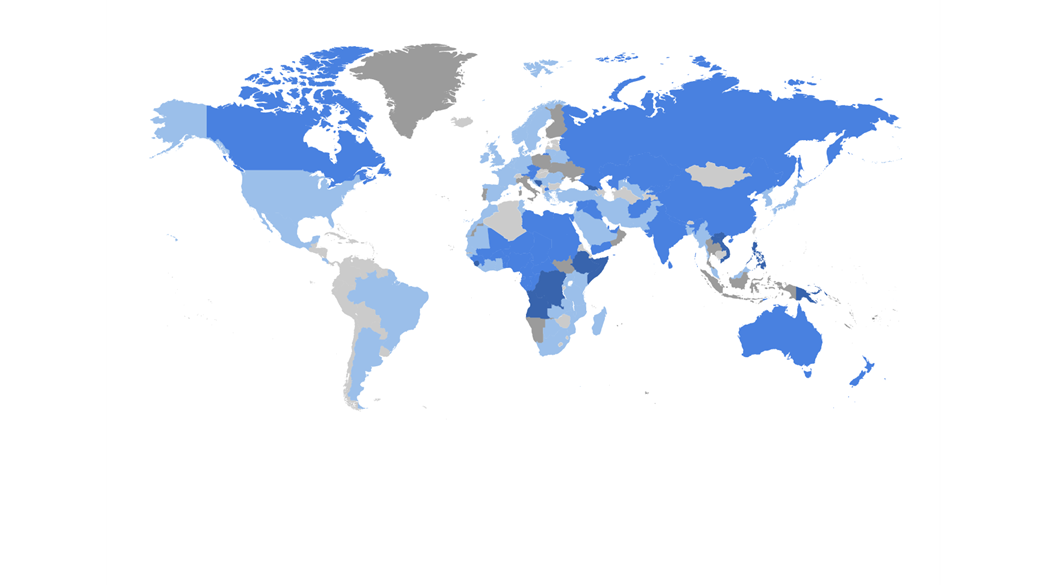
In 1974 whooping cough immunisation rates plummeted from 81% to 31% in England and Wales, resulting in epidemics.
Map: Museums Victoria
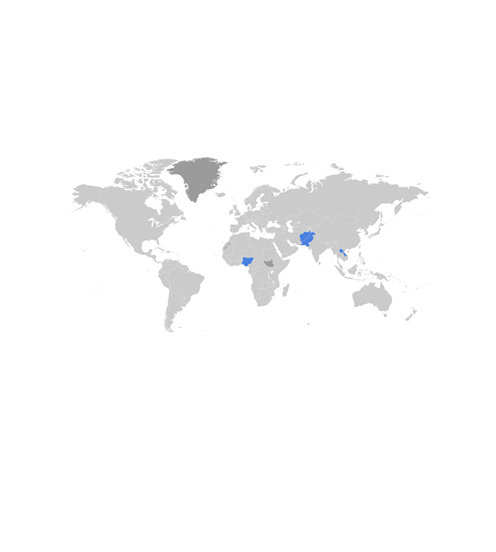
In 1990, more than 250,000 people died from whooping cough globally.
In 2010, Australia recorded more than 70,000 cases of whooping cough—among the highest in the world.
Because the virus has been allowed to circulate in a large population, it has given it the opportunity to mutate and adapt.
The vaccine that was designed to work against the previous strain is no longer as effective and a new one is now needed to get on top of it again.
Measles
Measles is another incredibly contagious disease recently targeted by anti-vaccine groups.
Before widespread vaccination began in the 1980s, about 2.6 million people died of the disease every year but in 2016 that number hit a record low of less than 90,000.
However, a failure to vaccinate children meant measles mortality climbed again in 2019.
Australia has a good track record with eliminating measles and has managed it several times, most recently in 2014.
‘Even a small decrease in vaccination rates can greatly influence infection,’ explains Dr Simkin.
‘Herd immunity is important for preventing future pandemics and protecting those too young, ill or allergic to be vaccinated.’
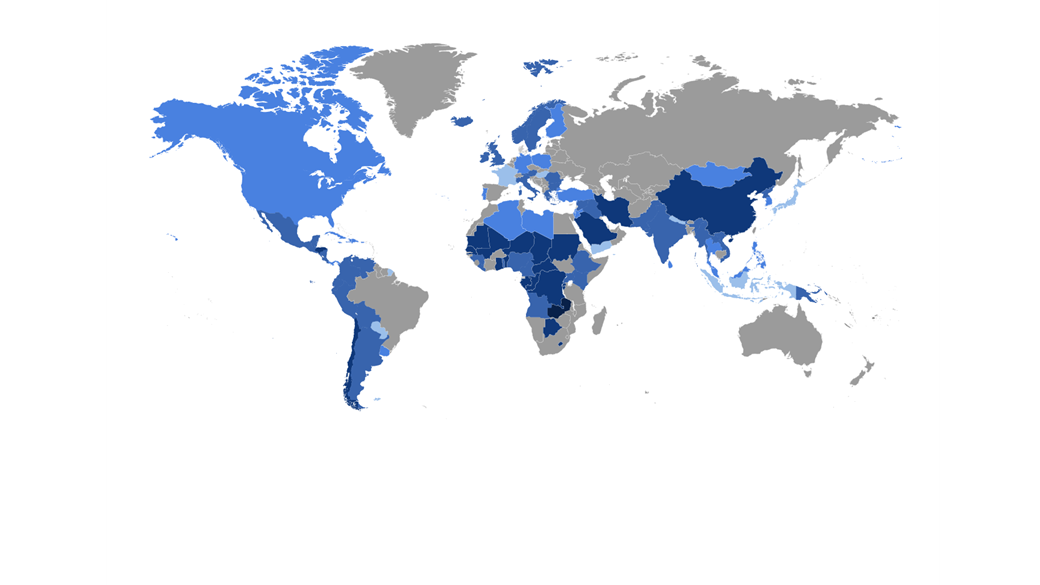
The tell-tale rash of measles is often accompanied by a high fever and cough. Source: Centers for Disease Control Photo: Jim Goodson/Centers for Disease Control/Public Health Image Library
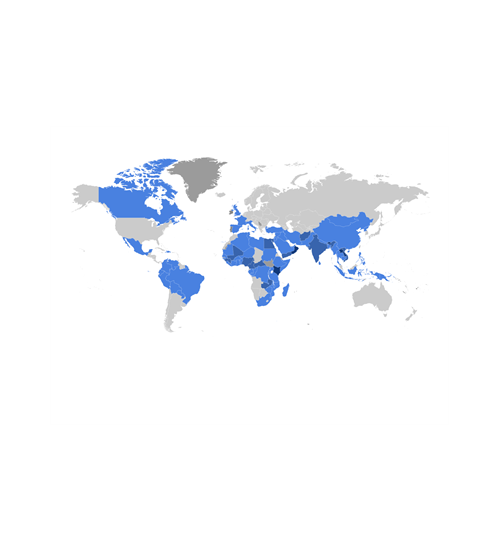
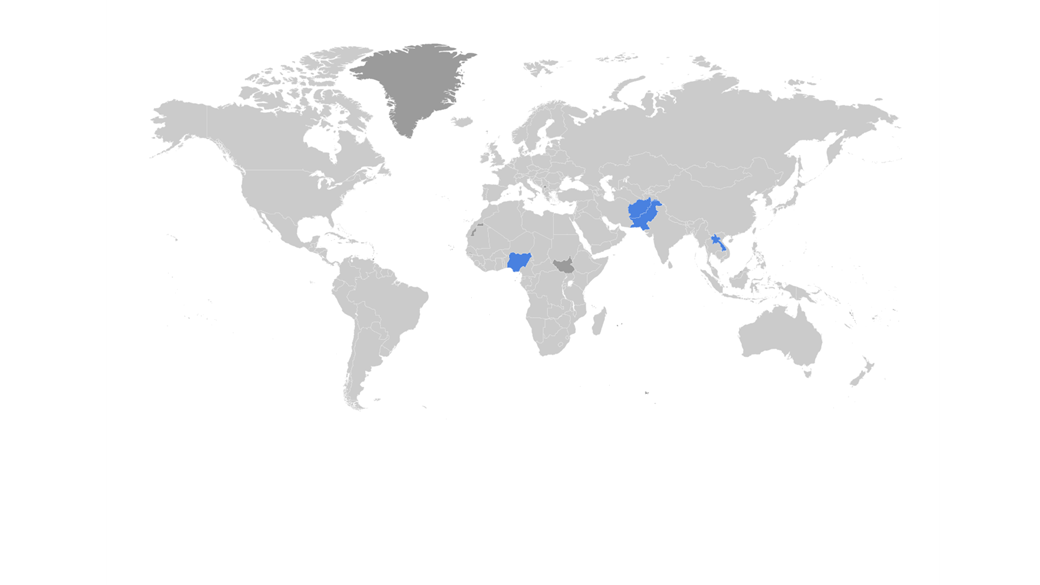
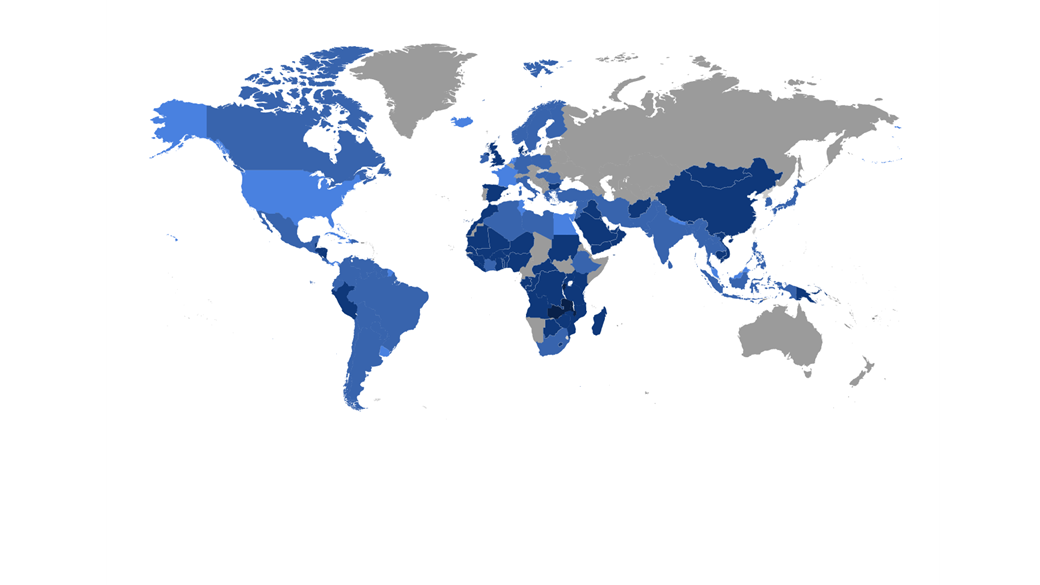
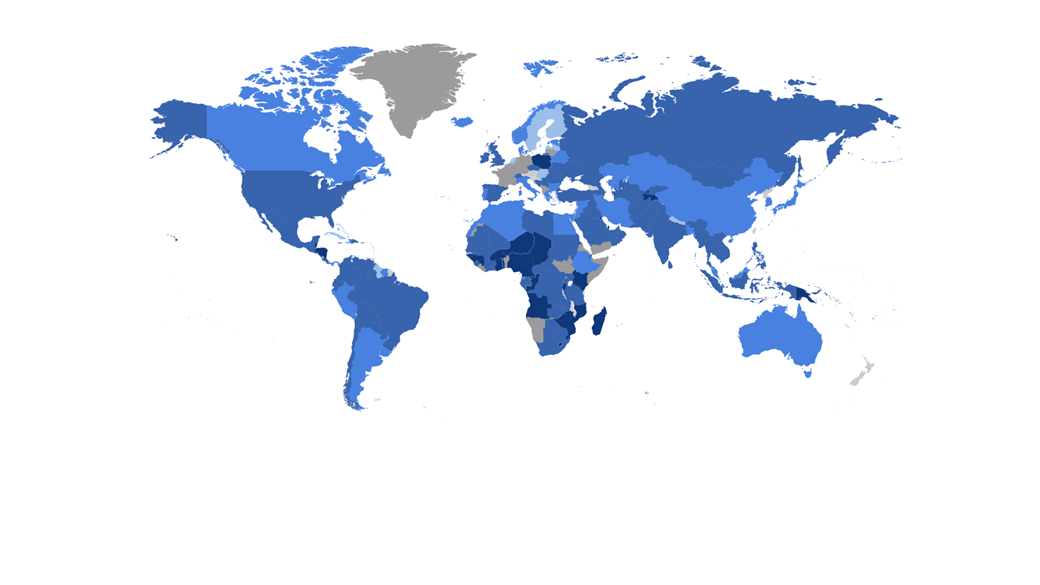
Before widespread vaccination began in 1980, measles killed 2.6 million people globally each year.
Map: Museums Victoria
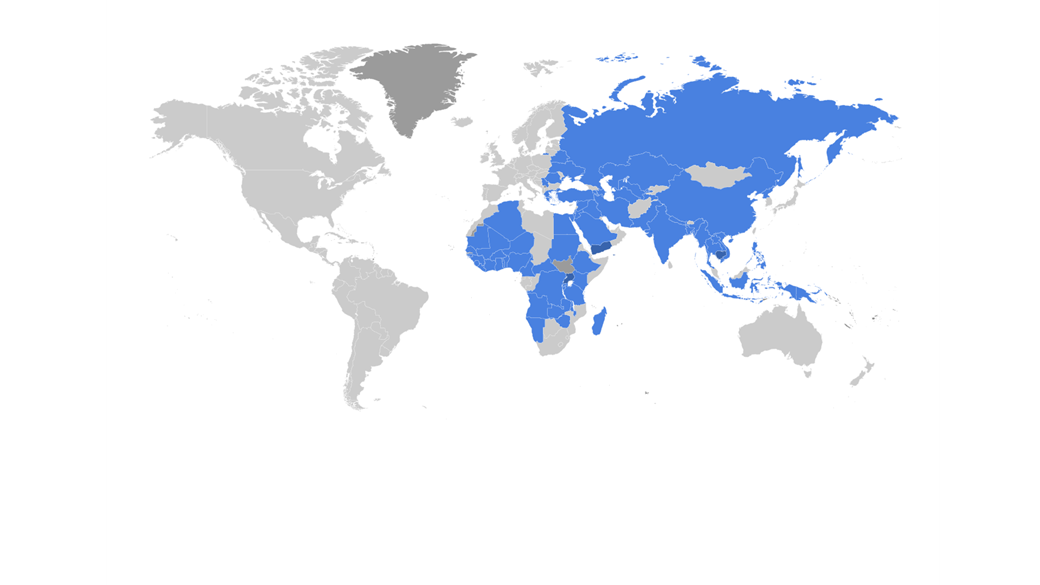
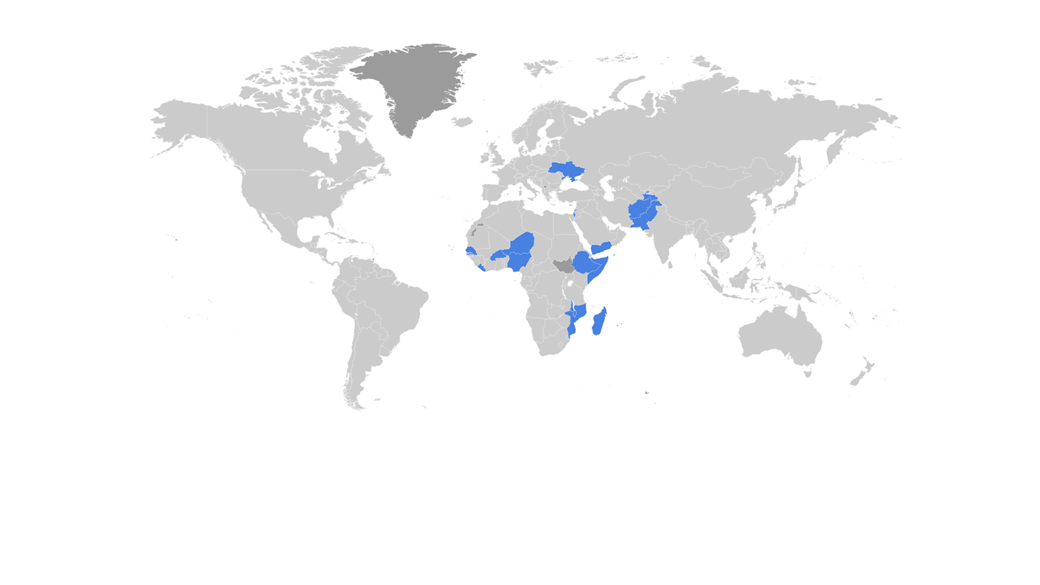
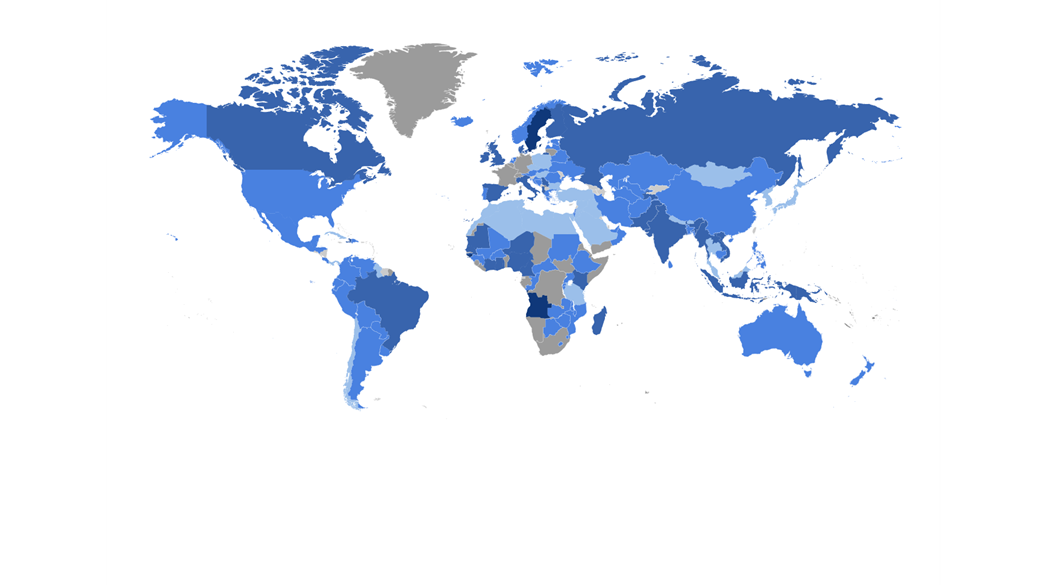
In 1990 global measles cases fell by two thirds from 1980 levels, to 1.3 million.
In 2014, Australia was declared free of circulating measles by the World Health Organisation. However, there have been more recent outbreaks traced back to infected overseas travellers.
While restrictions have stopped the spread of measles in Australia in 2021, the pandemic has also paused vaccination programs around the world—something that makes another measles outbreak all the more likely as things open up.
International research has also demonstrated a previously unknown danger of measles that has been dubbed ‘immune amnesia’.
These studies noted that after recovering from measles, there was a decrease in general antibodies (the proteins that flag germ invaders for destruction).
Some animal studies even showed a loss of B cells (which remember infections for fast future antibody production).
This immune amnesia could leave the sufferer vulnerable to other pathogens and was generally not seen in vaccinated groups.
All of this raises an important point—even if you do survive a disease, it does not mean you will be spared from long-lasting injury.
It is far better not to have the disease at all because many viruses cause damage to our bodies that can lead to other illnesses, sometimes years later.
This is the concept behind cancer vaccines, including for cervical cancer.
This vaccine does not target cancer at all, but rather the human papillomavirus (HPV) that can damage the body enough to increases the likelihood of cancer.
Lingering injury is also of concern with COVID-19 but because it is so new, we are not likely to see the long-term consequences for decades.
Coronavirus
Vaccine development for COVID-19 saw a number of firsts—one of which was the creation of several safe and effective options in such a short period of time.
‘It was a monumental human feat to develop the vaccine, test it and get it registered within two years,’ says Professor Pellegrini.
‘It’s never been done before.’
Part of the reason for that speed, explains Professor Pellegrini, is experience.
‘Several years ago we had what was called H1N1 flu, which really made us quite scared.’
The 2009 swine flu pandemic, caused by a relative of the H1N1 strain behind the 1918 flu, killed more than 150,000 people around the world.
‘It spread like wildfire, and we didn't respond very quickly,’ he says.
‘We learnt a little bit from that [H1N1] virus such that we did become a little bit more pandemic aware and a tiny bit more pandemic prepared.’
Professor Marc Pellegrini is an infectious diseases expert and leader of WEHI's COVID-19 research program. Image courtesy of WEHI.
The development of COVID-19 vaccinations also benefitted from all the development work that had gone before it, an established and well-funded industry, and collective focus.
The results of centuries of progress, housed in a tiny bottle. Photo: Eugene Hyland/Museums Victoria
‘This is what happens when we throw everything at creating a solution,’ says Dr Simkin.
Those developing COVID-19 vaccines were able to take advantage of a tried and tested method that relies on the outer coat of the coronavirus, also known as the spike protein.
‘If you consider the virus to be like a peanut, you take away the actual nuts inside and just have a little coat on the outside,’ explains Professor Pellegrini.
‘That little coat is actually an effective mechanism to educate the immune system.’
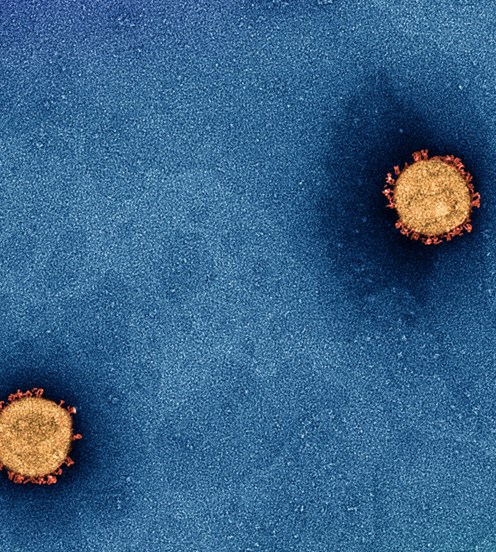
Here you can see the outer spike protein of the SARS-CoV-2 virus. It is this protein that allows the virus to get inside our cells. Image courtesy of the Doherty Institute. Photo: Photographer: Dr Jason Roberts; Electron Microscopist: Dr Andrew Leis/Copyright Doherty Institute for Infection and Immunity 2020
But making viral coats for vaccines is not a trivial matter.
‘Very recent, and very timely, advances in vaccine technologies provided a massive leapfrog enabling us to quickly create COVID-19 vaccines.’
The AstraZeneca vaccine uses a benign chimpanzee cold virus that has been engineered ‘to deliver the spike protein to our cells so that we learn to recognise and respond to the real threat,’ says Professor Pellegrini.
‘The other way that you can educate our bodies to respond to spike protein is to use what's called mRNA.’
mRNA (or messenger Ribonucleic Acid) has been studied for decades but COVID-19 is the first time it has been available in vaccines.
As Professor Pellegrini explains: ‘mRNA is actually part of our normal biology—our DNA chromosomes make RNA, which becomes the template for making all of our body’s critical proteins.’
While most other vaccines use an inactivated or weakened form of the virus (remember Salk and Sabin?), mRNA vaccines are instead coded to simulate it so there is no risk of infection.
HT 57089 –
Vaccine Vial—COVID-19, Pfizer, 22 Feb 2021
Our body recognises the mRNA in the vaccine, like Pfizer and Moderna, and uses it to make the spike protein.
‘We only make the spike protein for a tiny period—just long enough to instruct our bodies to develop immunity to it,’ says Professor Pellegrini.
‘The reason mRNA is short lived is because our bodies actively destroy it…therefore the mRNA doesn’t hang around to interfere with DNA at all.’
He says it has been so successful, that it will ‘become the new fundamental platform’ for all vaccines.
‘In fact, we’ll probably go backwards and start reinventing some of our original vaccines that aren’t so good, using this mRNA technology.’
But Professor Pellegrini says that does not mean that vaccines like AstraZeneca are now obsolete.
‘Some vaccines have got peculiar side effects—they are very rare, but they are still very tangible.
‘Some people might not be able to have an mRNA vaccine because they are allergic to a thing called PEG (Polyethylene Glycol), which is critical to multiplying the mRNA.
‘Others might have problems because they’ve got major clotting abnormalities and they can’t have the AstraZeneca vaccine.
‘Having more vaccines available means we can immunise a greater proportion of people and we can mix and match them going forwards to optimise immunity.’
And while Professor Pellegrini does not believe it is possible to eliminate COVID-19 entirely, he says the virus can be controlled with high rates of vaccination.
‘It's a matter of making a substantial part of the population immune to this particular virus so that it doesn't transmit particularly well and you’re really forcing the virus to change.
‘Over time it will encounter more and more resistance to its spread, to the point where it becomes very hard for it to spread unless it becomes something that's incredibly benign.
‘That's probably how covid will end up,’ says Professor Pellegrini.
But as we have learned, that will take time and a lot of vaccines.
Many public buildings became vaccination hubs in 2021, including the Melbourne Museum. Photo: Photographer: Eugene Hyland/Museums Victoria
Museums Victoria acknowledges the Wurundjeri Woi Wurrung and Boon Wurrung Bunurong peoples of the eastern Kulin Nations where we work, and First Peoples across Victoria and Australia.
First Peoples are advised that this site may contain voices, images, and names of people now passed and content of cultural significance.
Join the mailing list and get the latest from our Museums direct to your inbox.
We'd love to hear about your experience with our website. Our survey takes less than 10 minutes and entries go in a draw to win a $100 gift voucher at our online store!